Question: How do obesity and poor metabolic health impair immune system function?
Takeaway: Poor metabolic health leads to a chronic inflammatory state and impaired immune organ function, which then lead to deficiencies in both the innate and adaptive immune response. These findings reinforce previous research indicating obesity and the metabolic syndrome increase infectious disease vulnerability.
Research has repeatedly indicated obesity and the metabolic syndrome increase risk of infection, lead to poorer disease outcomes in response to infection, and reduce vaccine effectiveness (1). This 2016 paper reviews multiple mechanisms by which metabolic defects could contribute to immune system impairment.
The immune system consists of two systems that work in concert to coordinate disease response. The innate immune system, which includes monocytes and macrophages, provides a rapid, nonspecific response to potential threats via an inflammatory response (2). The adaptive immune system, which consists of B and T cells, supports immunological memory and allows the body to respond more effectively to repeated infections (3). Immune system defects can lead to an insufficient or excessive immune response, either of which can be harmful (4, 5).
Increased adipose tissue volume, as is seen with obesity, leads to increased inflammation, both directly and indirectly. Adipose tissue expands in adult humans primarily through hypertrophy (i.e., increasing the size of fat cells) rather than hyperplasia (i.e., generation of new fat cells). As adipose cells expand, various cellular responses lead to increased levels of inflammation within fat tissue (6). Inflammation is followed by leukocyte infiltration, with the share of white blood cells present in adipose tissue rising from 5% in healthy tissue to 50% in obese individuals (7). This inflamed, leukocyte-rich adipose tissue secretes other inflammatory compounds such as TNF-a and IL-6 (8). These same compounds may make insulin resistance — which led the adipose tissue to expand in the first place — worse as increased TNF-a inhibits glucose uptake within skeletal muscle cells (9). In other words, the inflammatory response to adipose tissue expansion (fattening) leads to further worsening of insulin resistance.
As the fat tissue expands and becomes insulin-resistant, additional fat is released into circulation, some of which is taken up by organs (10). Immune system organs — including the bone marrow, thymus, and spleen — can take on fat through this process, which is much like the gradual immune system organ fat accumulation associated with aging (11). Fat accumulation impairs organ function and thereby impairs the production, functionality, and integrity of developing immune cells (12).
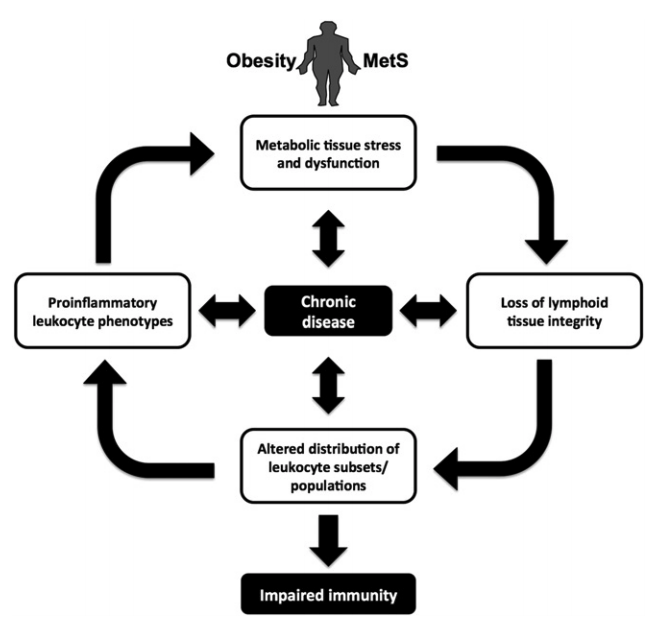
Figure 1: Summary of the mechanisms by which obesity, metabolic syndrome, impaired immune function, and chronic disease interact
One specific effect of these impairments is a reduction in the variety of circulating T-cells. This then leads to a reduction in the variety of pathogens to which the body can provide an effective immune response (13). Obese individuals, for example, show a reduced T-cell response to influenza virus infection and fail to maintain memory T-cells after infection. For similar reasons, vaccine failure rates are higher among obese individuals for the hepatitis B, tetanus, and flu vaccines (14). Across these and other conditions, obese individuals are more likely to have complications related to infectious disease and to require hospitalization (15).
The association between fat accumulation within immune organs and impaired immune function may explain the decline in immunity associated with aging. It may also explain the immune system benefits associated with fasting, caloric restriction, and similar dietary interventions (16).
Additionally, metabolic syndrome may impair immune function via secondary effects on HDL cholesterol. A growing body of research indicates HDL cholesterol plays a role in immune function and may help manage the inflammatory (innate) response to infection (17). Obesity and insulin resistance are associated with lower levels of HDL cholesterol and so may impair this element of the immune response. These and other mechanisms may also explain the increased rates of allergies (18) and cancer (19) in obese and metabolically unhealthy individuals, given the role immune system function plays in these conditions.
Notes
- Adipocyte dysfunctions linking obesity to insulin resistance and type 2 diabetes; Immunological complications of obesity; Normalization of obesity-associated insulin resistance through immunotherapy; Adipose tissue dysfunction in nascent metabolic syndrome; Adipose tissue dysregulation in patients with metabolic syndrome; The impact of obesity on immune response to infection and vaccine: an insight into plausible mechanisms; Obesity is associated with impaired immune response to influenza vaccination in humans; Obesity accelerates thymic aging; Circulating mononuclear cells in the obese are in a proinflammatory state; Lean, but not obese, fat is enriched for a unique population of regulatory T cells that affect metabolic parameters; Immunity, inflammation, and cancer
- Regulation of adaptive immunity by the innate immune system
- Evolving concepts of specificity in immune reactions; Memory CD4 T cells emerge from effector T-cell progenitor; Antigen-specific memory B cell development; Local development of effector and memory T helper cells; Pathogen recognition and inflammatory signaling in innate immune defenses
- Resolving inflammation: Dual anti-inflammatory and pro-resolution lipid mediators; The endoplasmic reticulum stress response in immunity and autoimmunity; The endoplasmic reticulum stress response in immunity and autoimmunity; Origin and physiological roles of inflammation
- An example of an insufficient response would be a failure to stimulate an inflammatory response when a pathogen is present. An example of an excessive response would be a nonspecific immune response (as in many autoimmune diseases) or a failure to bring levels of inflammation back to baseline once the pathogen has been eliminated.
- Adipocyte dysfunctions linking obesity to insulin resistance and type 2 diabetes; Lipolysis response to endoplasmic reticulum stress in adipose cells
- Monocyte chemoattractant protein 1 in obesity and insulin resistance; The immune cells in adipose tissue; Obesity is associated with macrophage accumulation in adipose tissue
- Long-term treatment with interleukin-1beta induces insulin resistance in murine and human adipocytes
- Tumor necrosis factor alpha produces insulin resistance in skeletal muscle by activation of inhibitor kappaB kinase in a p38 MAPK-dependent manner; Effect of tumor necrosis factor administration in vivo on lipoprotein lipase activity in various tissues of the rat; Tumor necrosis factor-alpha stimulates lipolysis in differentiated human adipocytes through activation of extracellular signal-related kinase and elevation of intracellular cAMP
- See previous references.
- Diet-induced obesity in mice reduces the maintenance of influenza-specific CD8+ memory T cells; T-cell recruitment and Th1 polarization in adipose tissue during diet-induced obesity in C57BL/6 mice; Obesity increases the production of proinflammatory mediators from adipose tissue T cells and compromises TCR repertoire diversity: implications for systemic inflammation and insulin resistance; Inhibition of thymic adipogenesis by caloric restriction is coupled with reduction in age-related thymic involution; Visceral fat accumulation induced by a high-fat diet causes the atrophy of mesenteric lymph nodes in obese mice; Impact of immune-metabolic interactions on age-related thymic demise and T cell senescence; Adipose-immune interactions during obesity and caloric restriction: Reciprocal mechanisms regulating immunity and health span; The immune system and aging: A review
- Journey through the thymus: Stromal guides for T-cell development and selection
- Obesity impairs lymphatic fluid transport and dendritic cell migration to lymph nodes; Obesity increases the production of proinflammatory mediators from adipose tissue T cells and compromises TCR repertoire diversity: Implications for systemic inflammation and insulin resistance
- Altered or impaired immune response to hepatitis B vaccine in WNIN/GR-Ob rat: An obese rat model with impaired glucose tolerance; Reduced tetanus antibody titers in overweight children; Obesity is associated with impaired immune response to influenza vaccination in humans
- Diabetes and the severity of pandemic influenza A (H1N1) infection; Relationship between community prevalence of obesity and associated behavioral factors and community rates of influenza-related hospitalizations in the United States
- Inhibition of thymic adipogenesis by caloric restriction is coupled with reduction in age-related thymic involution
- Acute inflammation and infection maintain circulating phospholipid levels and enhance lipopolysaccharide binding to plasma lipoproteins; The role of HDL in innate immunity; High-density lipoprotein cholesterol, size, particle number, and residual vascular risk after potent statin therapy; Dietary approaches to improving atheroprotective HDL functions; Chylomicrons enhance endotoxin excretion in bile; New roles of HDL in inflammation and hematopoiesis
- Association of obesity with IgE levels and allergy symptoms in children and adolescents: Results from the National Health and Nutrition Examination Survey 2005–2006
- Obesity and cancer risk: evidence, mechanisms, and recommendations; Innate and adaptive immune cells in the tumor microenvironment; Severe pulmonary metastasis in obese and diabetic mice
Comments on Impact of Obesity and Metabolic Syndrome on Immunity
Great article. Good to have insight in the immune system.
____
Traduction/résumé en français. Excusez les fautes d'orthographe :)
L’impact de l’obésité et du syndrome métabolique sur l’immunité
Question :
Comment l’obésité et une mauvaise santé métabolique impacté négativement la fonction du système immunitaire
Conclusion :
Une mauvaise santé métabolique mène à un état inflammatoire chronique et une fonction immunitaire des organes réduites ce qui provoquent à des déficiences aussi bien sur la réponse immunitaire innée qu’adaptative. Ces conclusions renforcent des études préalables indiquant que l’obésité et le syndrome métabolique augmentent la vulnérabilité aux maladies infectieuses.
____
Le système immunitaire consiste de deux systèmes qui fonctionnent en concert pour coordonner la réponse à la maladie.
Le système immunitaire innée amène une réponse rapide et non spécifique aux menaces potentielles via une réponse inflammatoire.
Le système immunitaire adaptif supporte la mémoire immunologique et permet au corps de répondre de manière plus effective à des infections répétées.
Un défaut de système immunitaire peut provoquer une réponse immunitaire insuffisante ou excessive et les deux peuvent être nocives.
Un volume de tissus adipeux augmenté, comme avec l’obésité, amène à une augmentation de l’inflammation aussi bien directement que indirectement.
Les tissus adipeux s’étendent chez l’humain adulte à travers l’hypertrophie (augmentation de la taille des cellules graisseuses) plutôt que par l’hyperplasia (génération de nouvelles cellules de gras).
Lorsque le tissu adipeux s’étend, plusieurs réactions cellulaires amènent à un niveau augmenté d’inflammation dans le tissu adipeux.
Inflammation est suivit d’une infiltration de leucocyte avec la portion de globules blancs présentent dans le tissu adipeux augmentant de 5% à 50% chez l’individuel obèse.
Ces tissus adipeux enflammés sécrètent des composés inflammatoires comme le TNF et l’IL-6.
Ces composés pourraient faire empirer la résistance à l’insuline (cette résistance étant déjà responsable de l’augmentation du tissu adipeux à la base) car plus de TNF inhibe l’absorption du glucose dans les cellules squelettiques.
En d’autres mots, la réponse inflammatoire à l’expansion du tissu adipeux amène à une dégradation de la résistance à l’insuline.
Avec l’agrandissement du tissu adipeux et la résistance à l’insuline, plus de gras passe dans la circulation avec une portion absorbée par des organes.
Les organes du système immunitaire (comme la moelle épinière, le thymus et la rate) peuvent absorber du gras dans ce process qui est très similaire à l’accumulation graduelle de gras associée au vieillissement.
Cette accumulation diminue la fonction des organes et donc empêche la production, fonctionnalité et intégrité du développement des cellules immunitaires.
L’un des effets est la réduction des cellules lymphocytes T. Cela amène à une réduction dans la variété des pathogènes auxquels le corps peut donner une réponse immunitaire effective.
Les individus obèses par exemple, montrent une réponse réduite en cellule T au virus influenceza et ne parvienne pas à maintenir la mémoire de ces cellules après infection.
Pour cette même raison, l’échec de la vaccination est plus récurrente chez les individus obèse pour l’hépatite B, le tétanos et le vaccin de la grippe.
Avec ces conditions, les individus obèses sont plus à même de développer des complications.
L’association entre accumulation de gras dans les organes immunitaires et une fonction immunitaire diminuée peut expliquer le déclin de l’immunité avec le vieillissement. Cela peut aussi explique les bénéfices sur le système immunitaire comme le jeune, la restriction calorique et les interventions diététiques.
De plus, le syndrome métabolique peut diminuer la fonction immunitaire à travers des effets secondaires sur le cholestérol HDL.
De plus en plus de recherches montrent que le cholestérol HDL joue un rôle dans la fonction immunitaire et peut aider à gérer la réponse inflammatoire à une infection.
L’obésité et la résistance à l’insuline sont associées à un niveau amoindri du cholestérol HDL et pourraient donc éliminer la réponse immunitaire.
Ceci ainsi que d’autres mécanismes peuvent aussi expliquer l’augmentation des allergies et du cancer chez les obèses et chez les personnes en mauvaise santé métabolique vu le rôle que joue la fonction du système immunitaire dans ces conditions.
Impact of Obesity and Metabolic Syndrome on Immunity
1