Question
What role does insulin resistance in skeletal muscle play in the development of fatty liver disease, obesity, and other elements of the metabolic syndrome?
Takeaway
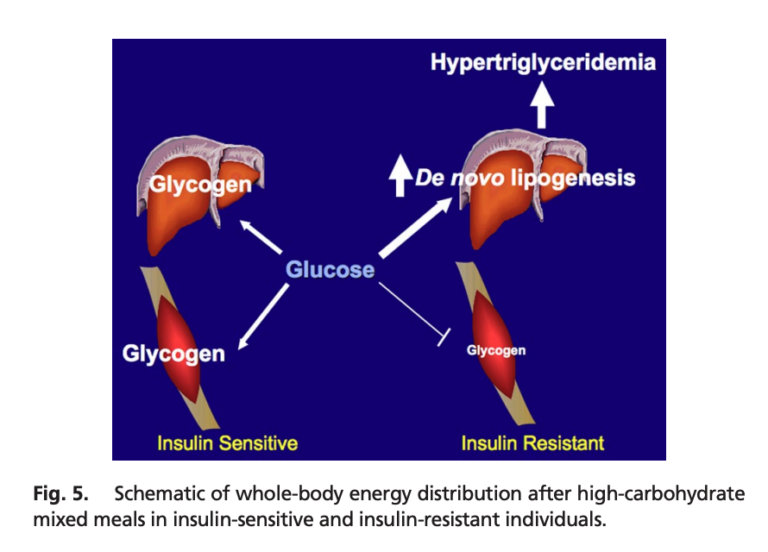
This small study indicates skeletal muscle insulin resistance may be the primary (initial) defect in metabolic deterioration. Insulin-resistant subjects, compared to matched, insulin-sensitive subjects, shuttled a larger share of ingested calories toward triglyceride production than glycogen storage. This shift, which occurred in subjects with normal weight and inflammation levels, would be expected to lead to increased liver and visceral fat storage, hepatic and peripheral insulin resistance, adiposity, and the other features of the metabolic syndrome. These results thus suggest muscular insulin resistance is the primary defect in the metabolic syndrome in at least some subjects, and further, that interventions to preserve or promote muscular insulin sensitivity may be particularly effective at preventing or reversing the metabolic syndrome.
In this 2007 study, 12 young, healthy, insulin-resistant men (1) were compared to 12 insulin-sensitive but otherwise similar men. Inflammation levels, weight, fat mass, and activity levels were similar between groups. The insulin-resistant subjects had lower baseline HDL, higher uric acid levels, and higher fasting plasma glucose, insulin, and triglyceride levels.
Both groups were given a high-carbohydrate meal (2). The subjects in both groups showed similar postprandial increases in blood glucose levels, while triglyceride and insulin levels increased more in insulin-resistant subjects than in their insulin-sensitive counterparts. Using labeled carbohydrates, researchers were able to track the fate of the ingested carbs. In the insulin-resistant subjects, muscle glycogen synthesis was 61% lower than in insulin-sensitive subjects; hepatic triglyceride synthesis and hepatic DNL were 2.5 and 2.2 times higher, respectively. In other words, a larger share of the ingested carbohydrates were shuttled toward triglyceride production rather than being stored as glycogen in insulin-resistant subjects.
Increased triglyceride production in insulin-resistant subjects accordingly led to higher levels of postprandial VLDL and lower levels of postprandial HDL than in insulin-sensitive subjects. This pattern is consistent with previous research indicating skeletal muscle insulin resistance leads to increased plasma triglycerides and reduced plasma HDL (3).
This study illustrates the primary role muscular insulin resistance can play in the development of metabolic disease. As shown here, muscular insulin resistance — observed prior to any defects in overall adiposity or inflammation — leads to a greater share of consumed calories being directed toward triglyceride production and a smaller share toward glycogen storage, even when identical meals are consumed. This increased triglyceride production would be expected to lead to fatty liver disease and hepatic insulin resistance (4), which itself leads to fasting hyperglycemia, obesity, and diabetes (5). The fact that these defects were visible in subjects with normal body weight and normal levels of inflammation suggests such factors are secondary defects and impaired muscular insulin sensitivity is the initial cause of the metabolic syndrome in at least some individuals (6). This suggests interventions to maintain and improve the ability of muscle cells to take up glucose in response to insulin — including, as previously reviewed on CrossFit.com, exercise — may play a particularly important role in the prevention and/or amelioration of the metabolic syndrome.
Comments on The Role of Skeletal Muscle Insulin Resistance in the Pathogenesis of the Metabolic Syndrome
8 Comments
Gerald Shulman’s group have done good work in identifying otherwise healthy young people who seem to have isolated skeletal muscle insulin resistance and who demonstrate biochemical features that might well predispose to type 2 diabetes, but I couldn’t find in this paper evidence that the subjects with skeletal muscle insulin resistance had family histories of type 2 DM. Have i missed it?
Dr. Kealey, I don't believe family Hx of T2D was part of the study's design. My read is consistent with yours.
This is another example of why the calorie paradigm is flawed: “As shown here, muscular insulin resistance — observed prior to any defects in overall adiposity or inflammation — leads to a greater share of consumed calories being directed toward triglyceride production and a smaller share toward glycogen storage, even when identical meals are consumed.”
I’m also struck by the connection here to the recent study (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6351883/) looking at metformin’s negative effect on exercise. While these studies are looking at different variables they are both considering how insulin sensitivity impacts the positive effects of exercise on muscle adaptation and thus overall health. The Metformin study’s lead author theorizes that it starts with the mitochondria.
I interview Adam Konopka, the lead author on this study and here’s an excerpt from our discussion.
Adam Konopka: Yes. So what you see in the skeletal muscle, maybe slightly different than what you would see in adipose tissue, or even perhaps the liver. Now, the thought process is that metformin has, at least in cell culture and animals, has been shown to actually lower mitochondrial function. It actually inhibits complex one, which is the first complex of the electron transport chain in the mitochondria. And so the thought is that it actually creates almost this kind of energetic stress. So if we’re inhibiting the mitochondria, we can’t produce maybe as much ATP or energy for our body to use. And by doing so we’re actually stimulating glucose uptake into the muscle because the muscle is almost, I don’t want to say starving, but it’s craving more fuel because we’re not producing as much ATP. And so that could be a good thing when you’re talking about a diabetic. But when we’re talking about exercise adaptations, if we’re inhibiting the mitochondria, our data would suggest that is actually why we are likely preventing some of these whole body adaptations. Our data show that at baseline mitochondrial function is highly correlated to insulin sensitivity. And then we also show after exercise training that there is a correlation with the change in mitochondrial function to the change in whole body insulin sensitivity.”
Here he is discussing the results of the intervention group that completed a 12 week exercise regime while taking metformin. The results surprised everyone.
Adam Konopka: “So the VO2 max, they did not improve as much and the insulin sensitivity, they did not improve at all. Yeah. And so these two factors are key in predicting mortality and morbidity. And so if metformin is preventing or attenuating the improvements in these physiological function, these physiological outcomes, that kind of raises some concerns if metformin should be prescribed to everyone for extending health span.
Elsewhere in the interview, he explains: “there’s a strong adaptation at the level of the skeletal muscle. And so you would expect a lot of improvements in different metabolic adaptations. At the level of the skeletal muscle where metformin’s primary tissue target is the liver. So you would think if you combine those two together, you would see adaptations at the level of skeletal muscle with exercise and then you get even better benefit with metformin by it’s targeting the liver. Both are involved with glucose regulation and insulin sensitivity. However, we didn’t see that. We actually saw that metformin completely blunted and prevented the improvement in insulin sensitivity, as measured by the oral glucose tolerance test. Although this is, I think this has grabbed a lot of people’s attention, there is precedent in the literature that other people have found this phenomenon as well.”
Emily, you mention this was an excerpt. Can we read the full interview somewhere?
The 2007 Shulman paper and the newer Konopka et al. paper are very important contributions and both need to be read by the audience of CrossFit.com. I'll point out that in our previous work, we found that the combination of exercise and metformin therapy lead to the most favorable postprandial glucose profile as measured by continuous glucose monitoring. https://www.ncbi.nlm.nih.gov/pubmed/28522762
Now, a few things warrant mentioning: Konopka et al. were looking at long term adaptations, whereas we assessed only acute responses. Moreover, in our study, we used a carbohydrate test meal to make the (subtle, or not so subtle, depending on your perspective) point that the mainstream dietary guidelines for T2D produced a ridiculous PPG response. Our data show that the best damage control is indeed the combination of walking exercise and metformin, in the acute setting at least. But, it would be better to avoid the glucose bolus altogether.
Nathan, I found the full interview here: https://empoweredhealthshow.com/metformin-cindi-morshead-adam-konopka/
And thanks for sharing your study, btw.
Hi Nathan - You can listen to the interview and view the full transcript on Empowered Health. I'm excited to look at your study too. Thanks for sharing. I do not think we really understand the mechanisms of action with regards to Metformin, and if you listen to that episode you'll hear the findings of Cindi Morshead who almost accidentally realized Metformin impacts females mice in positive ways that male mice do not benefit from which regards to brain injury. This is an incredible finding because it suggests there's a interplay between estrogen or other female hormones and the drug that heightens the benefits. Menopausal mice and male mice didn't see the effect. Thanks, Em
here's a bit from Morshead:
"it turns out that we were able to show that the STEM cells in an adult female brain are still responsive to metformin. They still can expand in number and promote differentiation into neural phenotype, into neural cells in a female brain, but they don’t expand a number in a male brain, so they’re non-responsive in the male brain. This is adults now. So you know, we were able to then take it one step further and go, maybe this is about the STEM cells and if it’s about the STEM cells, why doesn’t metformin activate male and female equally? Are the STEM cells different or is the environment of the brain different? And Rebecca was able to show that it’s actually the environment of the brain. The hormones in the female are able to modify the environment around a STEM cell to make them responsive to metformin and males, who do not have the female sex hormones obviously, they are non-responsive to the metformin. So the STEM cells themselves at the same in males and females, but the environment due to sex hormones is different and males cannot respond to the drug."
I think we can predict the problem with carb-loading. Now, what I would really love is to compare continuous glucose monitor (cgm) daily graphs in all these study participants.
I second that. It is interesting to note that normal glucose excursions were 140 post prandial. I’m thinking that is not physiologically normal and we should strive for under 140 and maybe even under 120. Even those insulin levels appear high and consistent with krafts definition of insulin resistance - even in the ones labeled normal