Diabetes is understood as a global disease, but there is no escaping the primacy of blood glucose and the effectiveness of dietary reduction. In some sense, there is nothing surprising about Hallberg et al.’s results, which are consistent with much work in the literature; they represent a breakthrough in their clear demonstration of point 1 of our review:
Point 1. Hyperglycemia is the most salient feature of diabetes. Dietary carbohydrate restriction has the greatest effect on decreasing blood glucose levels.
When Drugs Are not Enough
Drug advertisements or the insert in the package are likely to advise using the medication “when diet and exercise are not enough.” The idea that diet — or frequently, “lifestyle” changes — constitute the first approach to treating diabetes appears to be followed as much in the breach as in the observance. Critical is the implication that all dietary or lifestyle changes are the same, because this idea suggests little effort will be put into finding the limits after which drugs should be introduced. Point 11 from our review is relevant here:
Point 11. Patients with Type 2 diabetes on carbohydrate-restricted diets reduce and frequently eliminate medication. People with Type 1 usually require lower insulin.
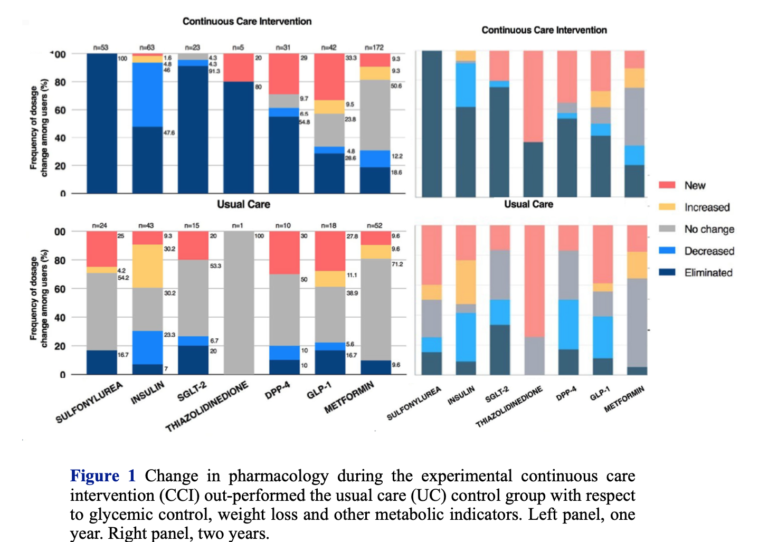
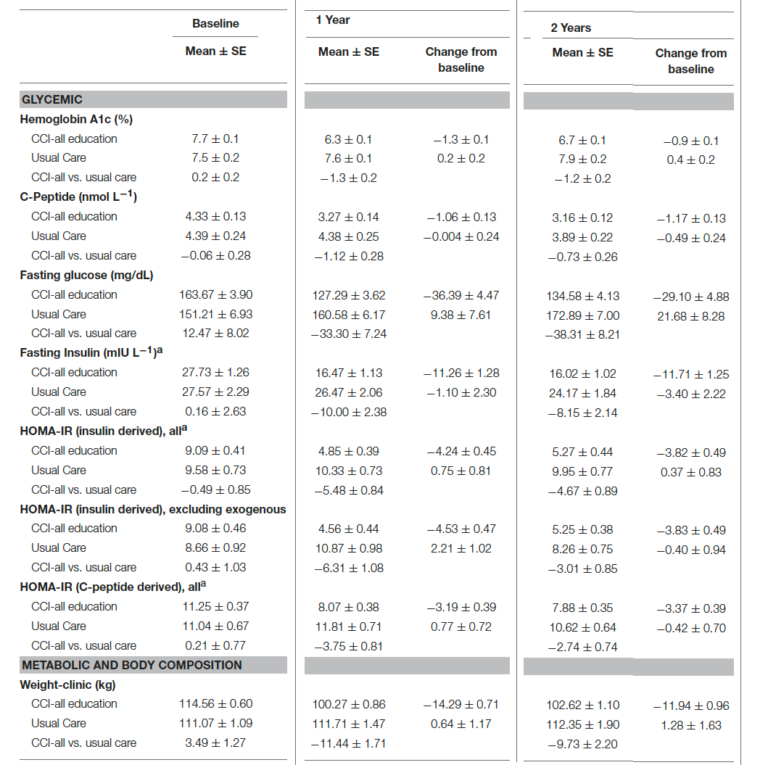
Drugs remain the mainstay of diabetes treatment, and despite the benefits, not needing a drug is always a sign of progress. Hallberg’s study (2, 3) shows that not all lifestyle changes are the same; overall, the low-carbohydrate/keto groups used half as many drugs as the control. A majority of the CCI participants (53.5%) met the criteria for diabetes reversal (meaning they were using only metformin). Another 17.6% achieved remission (i.e., requiring no medication). Of particular importance is the observation that 95% of people on insulin reduced or eliminated use.
Weight Loss
The resistance of the medical orthodoxy to the principle of carbohydrate restriction remains incomprehensible. In fact, one has to face the bizarre paradox that diabetes drugs are designed to reduce blood glucose in any number of ways while nutritional approaches and weight loss are considered primary, notwithstanding the universally accepted observation that many people with Type 2 diabetes are not fat and many overweight people do not develop diabetes. The insistence on weight loss is one of the objectionable aspects of traditional advice: It is, after all, not easy to lose weight, and emphasizing weight rather than glycemic control ensures lower probability of adherence and success. As point 3 of our review states:
Point 3. The benefits of dietary carbohydrate restriction do not require weight loss.
Weight loss protocols are usually designed to restrict calories across the board, which, because they usually start from high-carbohydrate baselines, de facto leads to reductions in carbohydrate. In any case, while the mechanisms are hotly debated, experimentally, low-carbohydrate diets almost always outperform low-fat diets, the usual alternative. A tabulation of RCTs in which the low-carbohydrate arm was under 35% of calories was published by the Public Health Coalition (Figure 2).
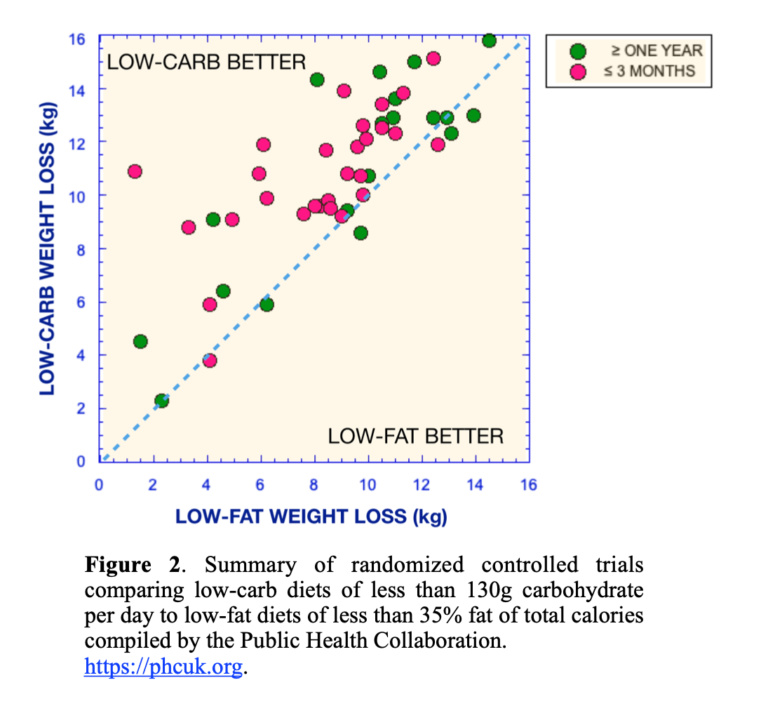
The mantra of nutritional medicine is that low-carbohydrate diets are better than low-fat diets in the short term but they are the same at one year. In a professional boxing title match, in the case of a draw, the champion maintains his crown. It is doubtful whether the low-fat diet is any kind of champion, but in fact, Figure 2 shows the argument against the low-carb diet is incorrect: While low-carbohydrate arm diets do better in the short term, they also do better after one year. The explanation of why this is not always seen is obvious and occasionally even stated explicitly. Adherence decays because of the looseness of the experiment protocol and the inability to monitor patient performance. The continuous care intervention of Hallberg et al., which takes advantage of telemedicine and personal counseling, dramatically increases persistent results, although there is some reduction in effects. Nonetheless, increasing adherence brings out the superiority of carbohydrate restriction. The principle, from point 4 in our review, is still:
Point 4. Although weight loss is not required for benefit, no dietary intervention is better than carbohydrate restriction for weight loss.
The ADA Vs. Science
“Low‑carbohydrate diets might seem to be a logical approach to lowering postprandial [after a meal] glucose,” said the American Diabetes Association (ADA) in a 2008 position statement (4). The comment was not meant as a guide to action. The statement continued: “However, foods that contain carbohydrate are important sources of energy, fiber, vitamins, and minerals and are important in dietary palatability. Therefore, these foods are important components of the diet for individuals with diabetes.” The confusion of carbohydrate, the nutrient, with foods that contain carbohydrate is deceptive and, in fact, odd in that energy is what the ADA always wants us to reduce. In any case, it is not just postprandial glucose. Improvement continues as long as dietary carbohydrate is kept low, which is perhaps why carbohydrate restriction, historically, was the recommended diet before the discovery of insulin.
Despite continued demonstrations of the expected efficacy of carbohydrate restriction, the 2018 ADA Standards of Care (5) indicated:
… a variety of eating patterns are acceptable for the management of diabetes (51, 53). The Mediterranean (54, 55), Dietary Approaches to Stop Hypertension (DASH) (56–58), and plant-based diets (59, 60) are all examples of healthful eating patterns …
The references the ADA cited were to summaries or reviews, but these did not include our 12 points of evidence review (1) or the “eating patterns” directly targeting blood glucose. Nor did the list include any low-carbohydrate or ketogenic approaches. There is no real explanation for this bizarre fear of carbohydrate restriction, but it remains widespread. The ADA holds unique responsibility for discouraging people from carbohydrate restriction, though the practice is pervasive. The Mayo Clinic, for example, offers the following recommendation:
Contrary to popular perception, there’s no specific diabetes diet. However, it’s important to center your diet around:
-
- Fewer calories
- Fewer refined carbohydrates, especially sweets
- Fewer foods containing saturated fats
- More vegetables and fruits
- More foods with fiber
A registered dietitian can help you put together a meal plan that fits your health goals, food preferences and lifestyle. He or she can also teach you how to monitor your carbohydrate intake and let you know about how many carbohydrates you need to eat with your meals and snacks to keep your blood sugar levels more stable.
Targeting sweets and “refined” carbohydrates is considered a step forward.
The ADA in 2019 and the Looming Dietary Guidelines
The ADA’s guidelines for 2019 received approbation for offering low-carbohydrate diets as one of the options (6). Some of us were not impressed. We found it scientifically inaccurate, rife with ambiguous language, intellectually lacking, tedious, repetitive, and full of empty, trivial statements. And, of course, there was no explanation as to what was wrong before. Hallberg and colleagues provided their own perspective on the lack of rigor (7), but there are numerous concerns. For instance, the guidelines claimed:
For people with type 2 diabetes or prediabetes, low-carbohydrate eating plans show potential to improve glycemia and lipid outcomes for up to 1 year (62–64, 86–89).
“Potential” is inaccurate and dishonest. Point 1 applies: Dietary carbohydrate restriction has the greatest effect on decreasing blood glucose levels.
Despite their inadequacy, like much current medical writing, the consensus statement in the ADA’s 2019 guidelines is self-congratulatory:
The authors of this report were chosen following a national call for experts to ensure diversity of the members both in professional interest and cultural background, including a person living with diabetes who served as a patient advocate.
And despite all this expertise:
An outside market research company was used to conduct the literature search and was paid using ADA funds.
Whose Diet Is This?
The 12 points of evidence in our review (1) made the case for carbohydrate restriction as the thing to try first. We were clear that the data were “proposed as the most well-established, least controversial results.” We continued: “We feel that these points are sufficiently strong that the burden of proof rests on critics. The points are, in any case, intended to serve as the basis for improved communication on this topic among researchers in the field, the medical community, and the organizations creating dietary guidelines.”
Oddly, although the ADA did not identify us by name, the 2019 guidelines seemed to have assumed there was somebody out there trying to insist on their own way of doing things and this somebody did not understand that different people might have different needs. The intro to the 2019 consensus statement (6), in its typically verbose way, pointed out:
Evidence suggests that there is not an ideal percentage of calories from carbohydrate, protein, and fat for all people with or at risk for diabetes; therefore, macronutrient distribution should be based on individualized assessment of current eating patterns, preferences, and metabolic goals. (my emphasis)
It is not clear that evidence can suggest there is not an ideal, only that the ideal hasn’t been found, but again, nobody claims there is an ideal amount of carbohydrates. The word “individualized” appears 18 times in the consensus report (6), simultaneously suggesting there are autocrats out there and relieving the ADA from making real recommendations. In fact, however, the novelty of Hallberg et al. (2, 3) lies in that it:
… utilizes continuous care through intensive, digitally enabled support including telemedicine access to a medical provider (physician or nurse practitioner), health coaching, nutrition and behavior change education and individualized care plans, biometric feedback, and peer support via an online community. (my emphasis)
With Hallberg et al.’s continuous care intervention:
Participants were provided individualized nutrition recommendations that allowed them to achieve and sustain nutritional ketosis with a goal of 0.5–3.0 mmol L-1 blood BHB. Participants were encouraged to report daily hunger, cravings, energy, and mood on a four-point Likert scale. These ratings and BHB (beta-hydroxybutyrate) concentrations were utilized to adjust nutritional guidance. (my emphasis)
Where Are We Now?
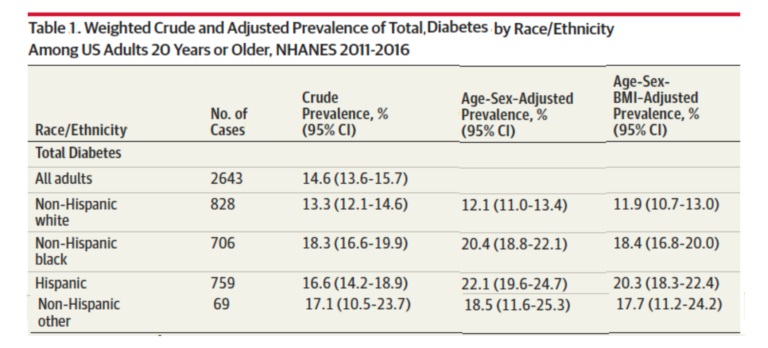
According to the Dec. 24 issue of JAMA (8), total diabetes (combined Types 1 and 2, diagnosed and undiagnosed (HbA1c > 6.5 %)) in the United States rests in the range of 14-22%, with significant differences based on race and ethnicity (Table 1 from reference 8). While described as an epidemic, the severity of the diseases appears to remain underappreciated, and public concern elicits nowhere near the same level of public response as diseases from infective agents (e.g., HIV or SARS).
Political pressure for reduction in the cost of drugs appears frequently, and there is particular outrage at the idea that people could die by virtue of not being able to afford insulin. While the drugs have varying degrees of efficacy, lip service at least is given to the importance of controlling dietary carbohydrate and, as noted above, proscriptions against sugar and “refined” carbohydrate are not likely to be useful if fear of fat prevails.
In the end, patients are on their own. Private and government health agencies continue to hold substantial power and, in some sense, the 12 points of evidence might be said to constitute articles of impeachment. Whether those in power will meet their critics remains to be seen.
Additional Reading
 Richard David Feinman, Ph.D., is a professor of cell biology at the State University of New York Downstate Medical Center in Brooklyn, where he has been a pioneer in incorporating nutrition into the biochemistry curriculum. A graduate of the University of Rochester and the University of Oregon, Dr. Feinman has published numerous scientific and popular papers. He is the founder and former co-editor-in-chief (2004–2009) of the journal Nutrition & Metabolism. He is currently researching the application of ketogenic diets to cancer.
Richard David Feinman, Ph.D., is a professor of cell biology at the State University of New York Downstate Medical Center in Brooklyn, where he has been a pioneer in incorporating nutrition into the biochemistry curriculum. A graduate of the University of Rochester and the University of Oregon, Dr. Feinman has published numerous scientific and popular papers. He is the founder and former co-editor-in-chief (2004–2009) of the journal Nutrition & Metabolism. He is currently researching the application of ketogenic diets to cancer.
References
- Feinman RD, Pogozelski WK, Astrup A, et al. Dietary carbohydrate restriction as the first approach in diabetes management: critical review and evidence base. Nutrition 31(2015):1–13.
- Hallberg, S.J., McKenzie, A.L., Williams, P.T. et al. Effectiveness and Safety of a Novel Care Model for the Management of Type 2 Diabetes at 1 Year: An Open-Label, Non-Randomized, Controlled Study. Diabetes Ther. 9(2018): 583–612
- Athinarayanan SJ, Adams RN, Hallberg SJ, et al. Long-term effects of a novel continuous remote care intervention including nutritional ketosis for the management of Type 2 diabetes: A 2-year non-randomized clinical trial. Front. Endocrinol. 10(2019): 348.
- American Diabetes Association. Nutrition recommendations and interventions for diabetes – 2008. Diabetes Care 31. Suppl 1(2008): S61-S78.
- American Diabetes Association. Chapter 4. Lifestyle management: Standards of medical care in diabetes – 2018. Diabetes Care 41. Suppl. 1(2018): S38–S50.
- American Diabetes Association. Standards of medical care in diabetes. Chapter 5: Lifestyle management. Diabetes Care 42(2019): S46-S60.
- Hallberg SJ, Dockter NE, Kushner JA, Athinarayanan SJ. Improving the scientific rigour of nutritional recommendations for adults with type 2 diabetes: A comprehensive review of the American Diabetes Association guideline-recommended eating patterns. Diabetes Obes Metab. 21(2019): 1769–1779.
- Cheng YL, Kanaya AM, Araneta MRG, et al. Prevalence of diabetes by race and ethnicity in the United States, 2011-2016. JAMA 322.24(Dec. 24, 2019): 2389-2398.
Comments on Diabetes and Carbohydrate Restriction: Where Are We Now?
6 Comments
Having cared for many diabetic patients with a low carb diet over decades in clinical practice, I can attest that in our n=many anecdotal archive there is nothing so gratifying as telling a diabetic patient to follow an appropriate, whole foods, low carb diet and that we'd be able to sharply reduce or stop altogether their medications in short order and seeing the joy of that success in their faces. There will be some people with DM1 of course that must continue to add a bit of insulin, but the amounts needed to cover the carb and protein intake on a low carb diet will be small numbers. And as our good friend, Dr. Bernstein, always points out, there is the error or large numbers. Drawing up units of insulin is not a precise science -- there is an error inherent in the process of maybe 10% or more. That error, that 10% of 5 units is very small, but of 50 units is very large. And the wild swings in blood sugar that it inspires will put the patient on their face unless they 'cover the insulin' with additional carb. On a carefully controlled low carb diet, for those patients on insulin, there's less chance for the 'error' to magnify and they'll stay in tighter control. The process is infinitely easier and smoother for the DM2 patients, who until they're pretty far gone, can gain complete control by changing what they eat. Then the price of insulin doesn't matter whatsoever because they will no longer need it. And for most, no oral hypoglycemics or antihypertensives either. How much better is that?? And who, who has ever taken the Hippocratic oath, would be opposed?
The 2015 article by Richard Feinman and his colleagues has borne well the test of time, for it anticipated the findings of Hallberg et al. Essentially, Feinman et al were and are right. But two points may perhaps be made. First, how can we reconcile the fact that there are two good ways of reversing type 2 DM? Namely a low CHO diet or or a weight loss diet (as so well described by Roy Taylor et al)? I think the answer is liver levels of triglyceride, which rise with overweight generally, but which rise particularly with CHO in the diet. That in turn precipitates glucose and insulin resistance.
Second, Richard Feinman is puzzled about the weight loss story: but Roy Taylor articulates the case for individual thresholds. As the population gets larger, so more individuals cross that threshold, but everyone's threshold is different.
oh, and a third point may be made. Feinman et al, like Taylor et al, are good scientists, in that they ignored conventional wisdom, they looked at the data dispassionately, and they constructed new paradigms. And they were brave in articulating their new paradigms--courage is as important to good science as it is to commercial entrepreneurs.
Terrence,
Thank you for sharing your thoughts. I looked up the Roy Taylor study and found it interesting. Here is a link to it: www.ncbi.nlm.nih.gov/pmc/articles/PMC6399621/
and a few passages I found compelling. Referring to the Couterpoint study:
The results were clear-cut: individuals with very ordinary type 2 diabetes (up to 4 years duration) regained absolutely normal fasting glucose levels within 7 days of commencing a very low calorie diet. This was despite stopping metformin therapy on day one of the diet. Liver fat levels dropped by 30% and liver insulin sensitivity returned to normal in the first 7 days, explaining the change in fasting plasma glucose. However, the change in insulin secretion followed a different time course, gradually improving to normal over 8 weeks.
The quote below refers to the Diabetes REmission Clinical Trial (DiRECT) study:
At 12 months, 24% achieved weight loss of more than 15 kg in the intervention group. 46% of the intervention group had non-diabetic HbA1c off all antihyperglycaemic agents. The underlying changes in intra-organ fat remained constant in those achieving remission. Remission primarily depended upon degree of weight loss, with achievement increasing steadily from (7%) with only 0–5 kg weight loss to 86% who lost 15 kg or more.
It goes on to mention exercise, which I assume to mean prolonged, low-intensity cardio:
Increase in exercise during the weight loss phase was discouraged as this tends to be accompanied by compensatory eating. This phenomenon explains why a portion of people fail to lose weight under conventional care.16 However, a steady increase in physical activity was strongly encouraged during weight maintenance. Recognition of this one-two approach for the very different phases of weight loss and weight maintenance is crucial.
This line in the Further Questions section is pretty cool (emphasis mine):
Publication of the Counterpoint study in 2011 elicited a major influx of enquiries from people with type 2 diabetes, and ‘how to do it?’ information was placed on a website.33 Subsequently, many individuals reported upon their own experience and 77 provided sufficient information to analyze.34 The majority were able to achieve normal glucose control having stopped their oral hypoglycaemic agents. Half of the group achieved this without medical help and in some cases against medical advice.”
Roy Taylor's diet, as I recall, is a starvation diet, 600-800 kcal, or about half the calories of the Minnesota Starvation experiment. My reaction when I first saw it was that it represented the lengths that people would go to, the extent to which they would subject patients to real suffering, just to not mention low carbohydrate diets. And I don't know how much Taylor and I are good scientists but good scientific practice dictates that you cite relevant evidence -- especially contradictory evidence -- in evaluating your results. You will not find references to any low-carbohydrate studies in the paper mentioned above by Tyler Hass, or I suspect in any other studies of Taylor's diet. As a control, Sarah Hallberg always says publicly that there are three ways to put DM2 in remission and cites Taylor's as the second (surgery is the third). As in my original post, the fact that weight loss is not required for improvement in glycemic and other features of diabetes (and nothing is more effective than low-carbohydrate diets for weight loss) stands as a challenge to Taylor's extreme dietary approach. He does not mention that challenge.
The real difference is that thousands if not millions of people pursue LCHF diets for diabetes. You can hear their stories on social media, a greatly underutilized resource (although Lennerz, et al. (Pediatrics. 2018;141:e20173349) are a start). I don't know what the record of Taylor's diet is outside of his clinical studies but I don't see popular experience and there is obvious bias, especially in the sins of omission.. Ironically, of course, sustainability is always the criticism of low-carb diets. How can anybody eat all that steak when they could do 800 kcal/day?
Of course, diabetes is a serious disease and if they can go through extreme caloric restriction it may be up to the patient. I would, however, counsel any such patient to talk to Mary Dan Eades first (comment below).
Dr. Feinman, in his characteristic understated fashion, touches on some very important points.
I just listened an interview of ADA CEO Ms. Tracey Brown, who is T2D in the past 16 years. First CEO with the actual decease -and with a continuous glucose monitor CGM.
She quitted with insulin and 3 pills; one is about to go this year. How come? She’s abandoned the rice, she tosses the hamburger buns, she reads the labels and googles restaurant foods nutritional values. Sounds like a low-carb lifestyle, or as she calls it, as diabetic you must pay attention to the carbs. I guess she is actively using her CGM meter and acting accordingly.
She even met with Dr. Bernstein last year! An ADA official, this must be new to them.
I think and hope this is going to lead somewhere, let’s see. The lady understands the connection in between eaten carb and glucose and insulin, and that avoiding carb is good for her.
Maybe these cautious baby steps described by Prof. Feinman shall grow longer... the prevention of prediabetes developing into T2D needs a milder version of T2D diet. Which has to address the right things and deviate from the "general recommendations".
Youtube video available at sisters4fitness, from last week. Kind of a "coming out"...
JR