Currently in the United States and across the world, most of our healthcare dollars (which make up a very large portion of our overall economy) are spent on chronic metabolic disease. Billions of additional dollars are spent and quality of life reduced due to the secondary effects of these metabolic diseases as well as sedentary lifestyles, diets high in ultra-processed foods, and the effects of isolation across our communities.
Patients come to physicians and other healthcare professionals seeking to preserve, improve, or restore their physical, mental, or emotional health. Although as professionals we are highly trained in the physiology and pathophysiology of human bodies as well as the science of human disease, ranging from the intricacies of microbiology and cell biology to pharmacology and surgical technique, there are gaps in our training with respect to the normal patterns of human behavior and physical training to optimize health. We are trained to use the lens of disease to view health, where the absence of disease is regarded as success rather than the presence of wellness — and much less often the presence of fitness. A handful of specialists (physical therapists, physical medicine and rehab specialists, and some orthopedic surgeons) may have some additional training in these topics, although their training is focused primarily on specific disease processes and recovery patterns. Often, the services they provide to patients are only for returning to some level of — but not full — recovery.
As physicians practicing primary care internal medicine and general neurology, we and our patients have benefitted from CrossFit training and education. Although we both initially pursued CrossFit for our own well-being, within months and increasingly over the years we have relied on our CrossFit educational experiences to educate our patients on improving their movement patterns, physical fitness, and metabolic and mental health.
In primary care family medicine and general internal medicine, we advise each and every patient to visit his or her physician for an annual wellness visit (AWV). The Affordable Care Act has mandated all payers (including Medicare and Medicaid) to cover the AWV. Utilizing evidence-based guidelines, patients are screened for metabolic disease according to their risk, based on age and other family history. Patients benefit from early detection of metabolic diseases such as diabetes, hypertension, and hyperlipidemia, as well as early cancer detection.
the missing prescription
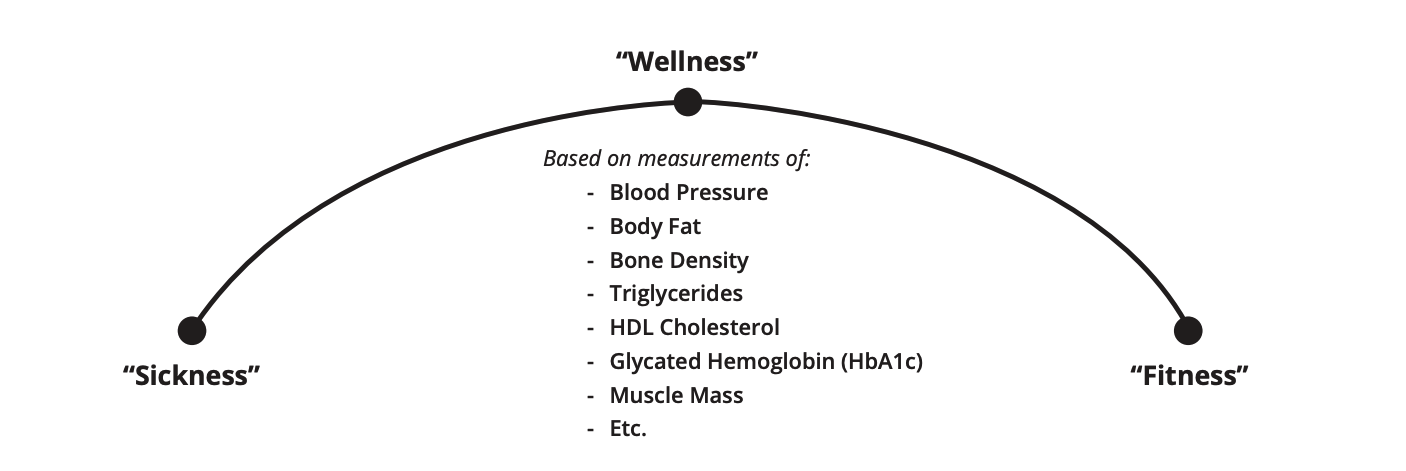
In CrossFit, we use the framework of the sickness-wellness-fitness continuum. The patients with abnormal findings at an AWV will fall between the sickness-wellness portion of the arc, but a large majority also land at wellness — all their metabolic values and blood-pressure measurements may be in the normal range; however, they are often very far from fitness. They may not be able to run a mile in under 15 minutes or deadlift even 50% of their body weight using proper form. Further, they do not meet the CDC guidelines for exercise for adults, they eat a diet high in processed foods, and they have a high percentage of fat in their body composition as well as a low percentage of muscle.
All the patients who land between sickness and wellness can benefit from more concrete advice to move them toward fitness. An experienced CrossFit coach can guide our patients in correct movement patterns and learning to exercise with intensity appropriate to their level. It’s incumbent upon us physicians to guide them to the methodology that can prevent and treat sickness.
2019 CDC Guidelines for Exercise for Adults recommend 150 minutes a week of moderate-intensity exercise and strength training twice a week. Recommendations for older adults specifically mention activities that promote balance. Further, in the notations, it is mentioned that 150 minutes a week of moderate-intensity exercise could also be 75 minutes a week of vigorous-intensity exercise.
Looking across the options available for our patients, it’s hard to find an “Rx” for exercise that more closely aligns with these guidelines than attending a CrossFit class one hour a day, four to six days a week. Perhaps some patients could supplement with one to two longer, moderate-intensity cardiovascular sessions depending on the week’s workouts. Often, patients need prolonged onboarding to have the prerequisites to move safely.
For example, Ms. Smith is an 88-year-old patient diagnosed with Alzheimer’s disease. Her daughter asks, “How can my mom improve her memory?” Cardiovascular activity has been shown to reduce the risk of developing dementia and improve memory in patients already diagnosed with dementia. Ms. Smith is deconditioned (or untrained) and needs help to stand and walks with a walker. Her journey to reaching CrossFit’s goal of metabolic conditioning requires a team, beginning with a physical therapist with a transition to a coach who can safely take her to extended periods of physical activity.
Even those of us in the CrossFit community who are aware of these guidelines and have experienced the CrossFit methodology in our own personal lives do not often feel confident to recommend a specific gym or program. This is where the CrossFit physician community can play an important role. Just as we take care to know which specialist physicians to refer our patients to, we need to take the time to get to know the affiliates, affiliate owners, and coaches in our communities. Taking the time to obtain the basic certifications ourselves (CF-L1 and CF-L2) will allow us to better guide our patients and assess specific gyms, programming, and coaches.
Coaches and affiliate owners also have an important role to play in this bilateral relationship. They should understand the importance of the annual wellness visit and why members should always take advantage of this benefit. A patient with undiagnosed metabolic or endocrine disease is unlikely to be able to fully benefit from their time in the gym, and this may lead to discouragement and quitting.
As we look ahead to bringing the benefits of CrossFit to our patients, we need to add some additional “vital signs” to their AWVs — such as their mile time, deadlift weight, and depth of air squat. (In the case of Ms. Smith, her first “vital sign” was to stand from her chair with her legs using her arms for support five times. On her second visit, her goal was 3 rounds for time of 5 stand-ups and sit-downs from a chair with a 50-foot walk. Her goals will incrementally increase to 10 minutes of as many reps as possible of a scaled air squat and brisk walking before a new goal is set.)
Addressing Common Misconceptions
It’s incredibly important for physicians to be equipped to address common misconceptions regarding CrossFit. In particular, the perception that CrossFit is dangerous for the average individual. This topic has been addressed in multiple forums, including online articles from CrossFit and others, podcasts, and social-media posts and comments. While another entire article could be written on this topic, we would like to emphasize a few points here.
- Physicians should inform patients that the core of CrossFit methodology emphasizes mechanics, consistency, THEN intensity. If a patient encounters a coach who is encouraging higher loads without proper emphasis on mechanics first, the patient should seek a new coach and/or inform the affiliate’s owner of the experience with the coach.
- Ego has no place in the CrossFit affiliate. Egotistical loading of the bar and/or disregard of coach corrections will increase the risk for injury. While the CrossFit methodology encourages measuring time and recording loads, ultimately, outside of elite competition, the main purpose of logging these values is to encourage one another in the gym and to track individual progress over time.
- Every physical activity has some risk of injury. In fact, statistics have consistently shown that exercise in a CrossFit affiliate is one of the least likely activities to result in injury relative to many other common sports. No physician would tell a patient “never go running,” and CrossFit should be held to the same standard. A superb resource is the CrossFit Health presentation by Dr. Amy West (CFMD-L2).
- Some chronic or acute injuries will require modifications to prescribed workout movements. CrossFit physicians should remain available to patients to advise them on modifications and/or refer them to a qualified physical therapist or specialist.
Preventable and treatable chronic diseases are rampantly decreasing quality of life while simultaneously ending lives early. Our job as physicians and CrossFit coaches is to fight that tide — and if we do it together, we just might succeed.