Eleven diabetic women were instructed to follow a ketogenic diet for 90 days. Dietary instructions were simple: Reduce carbohydrate intake to less than 30 grams per day while consuming ~20% of calories from protein and the remainder from fat. Ketone levels were tested weekly, with all 11 women successfully maintaining at least mild ketosis (i.e., detectable elevation of blood ketone levels, indicative of at least some adherence to the KD) for the duration of the study.
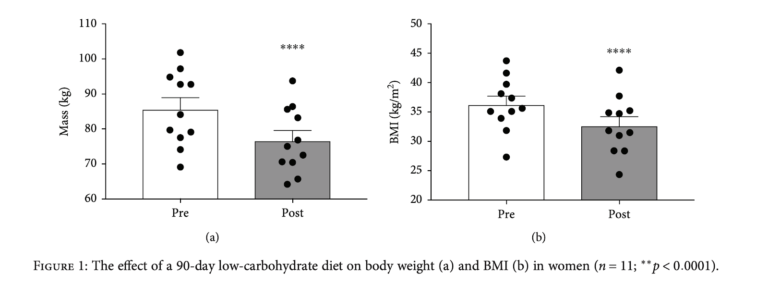
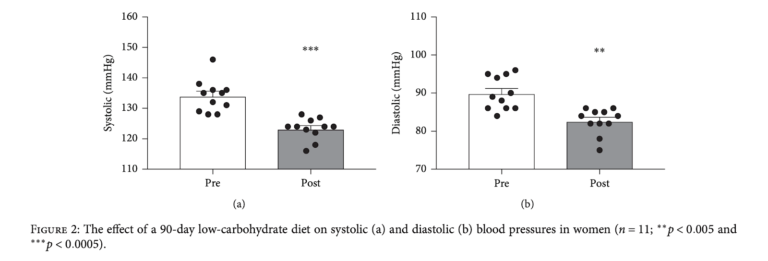
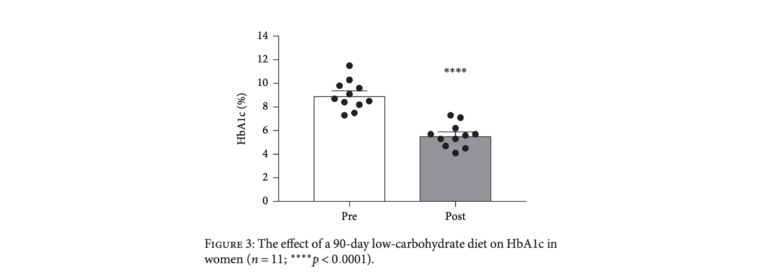
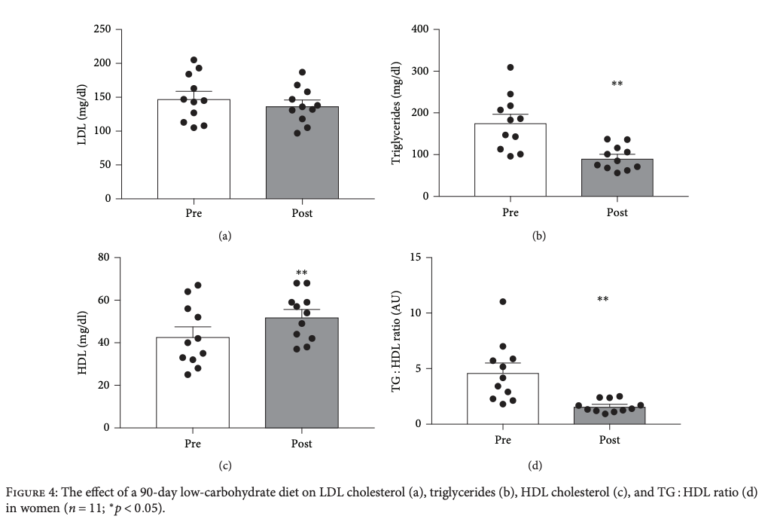
All 11 women lost weight, with an average weight loss of 9 kg. HbA1c decreased dramatically, from an average baseline of 8.9% to 5.6% at 90 days. Nine of the 11 women completed the study with an HbA1c below the cutoff for a diabetes diagnosis (6.5%). Improvements in multiple cardiovascular risk factors were also observed, including a decrease in blood pressure, an increase in HDL cholesterol (43.1 to 52.3 mg/dL), and a dramatic decrease in triglycerides (177.0 to 92.1 mg/dL). Both individual and group changes are summarized in the figures below.
In total, these results indicate a very low-carbohydrate ketogenic diet can reverse diabetes while driving substantial weight loss and reducing heart disease risk within 90 days. When compared to existing therapies, such as insulin secretagogues, this suggests the ketogenic diet is both more efficacious and has fewer negative side effects than pharmacological alternatives for diabetes treatment.