Parkinson’s disease is a chronic, progressive neurodegenerative disorder that primarily affects movement but ultimately involves multiple systems throughout the body. It is the second-most common neurodegenerative disease worldwide (Alzheimer’s being the most common), and its prevalence increases with age (De Sena et al., 2023). Although it is often recognized by its motor features such as shaking, stiffness, and loss of balance, Parkinson’s disease is biologically complex and extends well beyond tremor.
The disease is characterized by the gradual loss of brain cells that produce dopamine — a chemical that aids in controlling movement — gradually dying. These cells are located in a small region of the brain called the substantia nigra pars compacta (an area in the midbrain). As these neurons degenerate, dopamine levels decline within basal ganglia circuits that regulate movement. Because dopamine is essential for smooth, coordinated motor control, its depletion leads to symptoms including bradykinesia (slowed movement), rigidity (muscle stiffness), resting tremor, and difficulty with posture and stability. Nonmotor symptoms such as sleep disturbance, autonomic dysfunction, pain, mood disorders, and fatigue frequently accompany motor decline. Together, these impairments reduce functional capacity, diminish quality of life, and increase morbidity and mortality risk (De Sena et al., 2023).
Current treatment strategies aim to restore or mimic dopamine function and manage both motor and nonmotor symptoms. These approaches include pharmacologic therapy, surgical interventions such as deep brain stimulation, and multidisciplinary supportive care that includes physiotherapy, occupational therapy, speech-language therapy, nutrition support, and mental health care. While effective for symptom control, these treatments do not fully halt neurodegeneration, underscoring the need for adjunctive strategies that support neural health (De Sena et al., 2023). Exercise has emerged as a foundational lifestyle intervention in Parkinson’s disease management. Current guidelines from the Parkinson’s Foundation and the American College of Sports Medicine recommend at least 150 minutes per week of moderate to vigorous exercise, including aerobic, strength, balance, and flexibility components (Kathia et al., 2024).
Individuals with Parkinson’s disease frequently demonstrate reduced cardiorespiratory fitness, particularly in moderate to advanced stages, largely due to decreased physical activity levels. Aerobic training reliably improves maximal oxygen uptake, yet its effect on motor symptom severity has been variable, suggesting that exercise intensity may be a key determinant of effectiveness for the patient (Kathia et al., 2024). Moderate- to high-intensity exercise performed consistently over several months has been associated with reductions in motor severity and improvements in functional outcomes; however, these findings, derived from a small, proof-of-concept study without a non-exercise control group, support the need for further testing in larger (adequately powered), randomized controlled trials (de Laat et al., 2024).
High-intensity interval training, characterized by repeated efforts above 70 percent of peak oxygen consumption separated by brief recovery periods, has gained particular attention. Higher-intensity exercise may stimulate greater neuroplastic adaptations and produce more meaningful improvements in motor performance compared with low- or moderate-intensity training (De Sena et al., 2023). Neuroplasticity refers to the brain and nervous system’s ability to change its structure and function by forming, strengthening, weakening, or reorganizing neural connections. It’s the mechanism behind learning, memory, skill acquisition, and repair after many types of damage, including Parkinson’s disease. Improvements in cardiorespiratory fitness are especially relevant, as VO₂ peak is strongly associated with functional independence and long-term health outcomes, and may be relevant for resilience in PD.
This intensity-based model closely reflects the structure of CrossFit programming. CrossFit-style training regularly incorporates short, repeated bouts of relatively high-intensity functional movements, scaled to individual capacity, and integrates aerobic conditioning, resistance training, balance, and coordination. Importantly, prior research in adults has demonstrated that participation in CrossFit training twice per week for nine months significantly improved VO₂ peak (Schlie et al., 2023). These findings suggest that CrossFit methodology is capable of meaningfully improving cardiorespiratory fitness, a variable strongly implicated in Parkinson’s disease progression and overall health.
By delivering scalable high-intensity intervals within a supervised, community-based setting, CrossFit may provide a physiologic stimulus aligned with emerging evidence on exercise intensity and neuroplasticity — the brain’s ability to reorganize, adapt, and strengthen neural connections in response to activity and experience. In Parkinson’s disease, exercise-induced neuroplasticity may help support dopamine signaling and motor control pathways that become impaired as the disease progresses. As such, CrossFit represents a plausible and structured intervention framework.
Now, let’s dive into the current literature to see what insights can be gained from this fascinating area of research.
Feasibility and effect of high-intensity training on the progression of motor symptoms in adult individuals with Parkinson’s disease: A systematic review and meta-analysis. PLOS ONE
This systematic review and meta-analysis, conducted according to Cochrane and PRISMA guidelines and registered in PROSPERO, evaluated the effects of high-intensity exercise in individuals with Parkinson’s disease. Of 3,159 initially identified articles, 15 randomized controlled trials met inclusion criteria after rigorous screening and eligibility assessment. The included studies varied in exercise modality and design, but all incorporated high-intensity training protocols. Interventions included cycling, treadmill walking or jogging, and combined formats integrating strength, power, balance, flexibility, and functional training. Most studies compared high-intensity training with moderate-intensity exercise, low-intensity exercise, usual care, or control groups.
Across studies, high-intensity exercise was associated with meaningful physiological benefits and improvements in health, function, and quality of life. Four low-risk-of-bias trials, including 164 participants demonstrated a statistically significant improvement in maximal oxygen consumption, or VO₂ peak, favoring high-intensity exercise over control conditions. VO₂ peak is considered the gold standard measure of cardiorespiratory fitness and reflects an individual’s capacity to sustain moderate to high-intensity activity. Improvements in VO₂ peak are clinically relevant, as cardiorespiratory fitness is strongly associated with functional independence, morbidity risk, and treatment responsiveness in chronic disease populations. Even though the studies were quite different from each other (heterogeneous) and overall certainty of evidence was rated low, the direction of effect consistently favored high-intensity training.
In addition to physiological improvements, high-intensity exercise produced significant gains in quality of life when compared to no-exercise controls. This is particularly important in Parkinson’s disease, where depression, cognitive decline, and progressive functional impairment substantially diminish well-being. Exercise appears to serve as a meaningful adjunct to clinical treatment by mitigating some of these psychosocial and cognitive burdens.
Mechanistically, high-intensity exercise demonstrated a greater effect on brain-derived neurotrophic factor, or BDNF, compared with moderate-intensity exercise. BDNF plays a central role in neuroplasticity and neuroprotection. Described as “miracle gro” for the brain, it supports neuronal survival, promotes synaptic adaptability, and may help preserve dopaminergic neurons that are progressively lost in Parkinson’s disease. Circulating BDNF levels increased following high-intensity training, which suggests that exercise intensity may influence not only motor symptoms but also underlying neurobiological processes.
Although variability in study design and methodological limitations were noted across trials, the collective findings provide support for the potential role of high-intensity exercise in individuals with Parkinson’s disease. At the same time, evidence suggests that physical activity across a range of intensities may confer benefit, reinforcing the importance of exercise as an integral component of comprehensive Parkinson’s disease management.
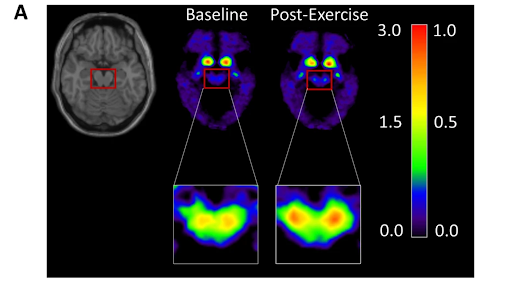
Intense exercise increases dopamine transporter and neuromelanin concentrations in the substantia nigra in Parkinson’s disease. npj Parkinson’s Disease
This proof-of-concept study investigated whether six months of sustained high-intensity exercise could induce measurable brain changes in individuals with mild, early-stage Parkinson’s disease. Participants were recruited from a movement disorders clinic and specialized Parkinson’s exercise programs. Only individuals within four years of diagnosis and without significant cognitive impairment were enrolled in order to maximize the ability to detect neurological change. After a two-week trial period to ensure adherence and safety, participants completed a structured six-month, high-intensity training program. Clinical assessments, motor testing in the medication “off” state, cognitive evaluations, and advanced neuroimaging were performed before and after the intervention. Heart rate monitoring confirmed that participants frequently exercised at moderate-to-high intensities, often reaching 70 to 80 percent of predicted maximum heart rate.
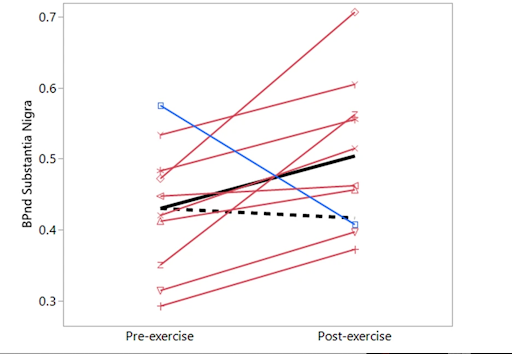
Following six months of training, significant neurobiological changes were observed. Dopamine transporter availability increased in the substantia nigra in 90 percent of participants. This finding is particularly striking because individuals with early Parkinson’s disease typically demonstrate substantial annual declines in dopamine transporter availability. Smaller and less consistent increases were observed in the putamen and caudate areas of the brain, but importantly, the expected decline in striatal regions was not seen. Neuromelanin-sensitive MRI also demonstrated an increase in neuromelanin signal within the substantia nigra pars compacta. Neuromelanin (similar in concept to the melanin in your skin) is a dark pigment found inside certain brain cells, especially those that produce dopamine in areas of the brain like the substantia nigra. In early Parkinson’s disease, neuromelanin levels typically decline rapidly, and the loss of these pigmented neurons as the disease progresses is what gives the substantia nigra its “pale” appearance at autopsy. The observed increase in neuromelanin, therefore represented a reversal of the anticipated disease trajectory.
Dopamine transporter proteins play a central role in maintaining dopamine storage and regulating dopaminergic signaling. Progressive reductions in transporter availability are a marker of disease progression. The increase observed after exercise may reflect improved functionality and metabolic activity of surviving dopaminergic neurons rather than structural regeneration. This interpretation is supported by the absence of motor worsening, stable clinician-rated disease severity (using MDS-UPDRS-III scores), and no increase in levodopa dosage throughout the study period. In a subset of participants followed for one year, motor scores remained stable, suggesting a sustained clinical benefit.
Neuromelanin has a dual biological role. When contained intracellularly, it may protect neurons from oxidative stress. The increase in neuromelanin signal observed after exercise may therefore indicate enhanced neuronal health or metabolic activity within remaining dopamine-producing cells. Taken together, the imaging findings suggest that intense exercise may exert neuromodulatory effects on the dopaminergic system and potentially slow or counter aspects of early neurodegeneration.
Although the study was limited by the absence of a nonexercise control group and a relatively small, highly motivated cohort, the consistency of dopamine transporter increases across participants makes a chance finding unlikely. Overall, the results provide in vivo evidence that sustained high-intensity exercise can induce measurable changes in brain biomarkers associated with Parkinson’s disease. These findings support the inclusion of structured, sufficiently intense exercise early in treatment plans and position exercise as a promising noninvasive neuromodulatory strategy deserving of larger randomized controlled trials.
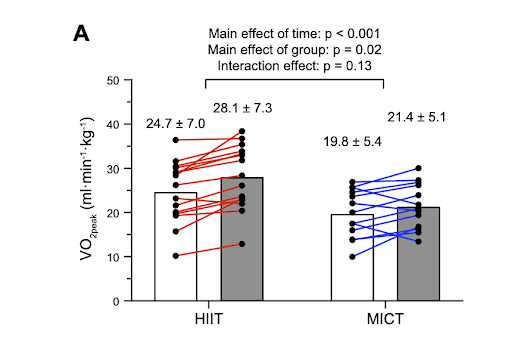
High-intensity interval versus moderate-intensity continuous cycling training in Parkinson’s disease: A randomized trial. Journal of Applied Physiology
This randomized trial compared 10 weeks of high-intensity interval training and moderate-intensity continuous training in individuals with Parkinson’s disease to determine whether exercise intensity meaningfully alters physiological and motor outcomes. Both groups improved cardiorespiratory fitness and demonstrated improvements in motor symptoms and subjective fatigue. However, high-intensity interval training produced a larger, clinically meaningful increase in maximal oxygen uptake despite requiring less total exercise time.
Although statistical differences between groups did not always reach significance, the magnitude of improvement favored high-intensity training. Participants in the interval group experienced an increase in VO₂peak that was approximately 2.2 times greater than that observed in the continuous training group. When applying established thresholds for clinically meaningful change, a greater proportion of participants in the high-intensity group achieved improvements exceeding both 1.5 and 3.0 mL·kg⁻¹·min⁻¹. Notably, these gains occurred without measurable changes in gait metrics, suggesting that improvements in cardiorespiratory fitness were independent of efficiency gained through mechanical walking adaptations.
The interval protocol consisted of repeated one-minute efforts at approximately 90 percent of peak power output, separated by one-minute recovery periods. In contrast, the continuous group cycled for longer durations at approximately 60 percent of peak power output, consistent with traditional moderate-intensity prescriptions. Importantly, participants in the interval group achieved near-maximal intensities that are difficult to sustain during steady-state exercise, while spending less overall time exercising.
These findings are clinically relevant because cardiorespiratory fitness is independently associated with mortality risk and overall health outcomes. The greater relative improvement in VO₂peak observed with high-intensity intervals suggests that this format may confer amplified physiological benefit in Parkinson’s disease. Moreover, interval training may be more time-efficient and potentially more tolerable for individuals who struggle to sustain prolonged continuous exercise due to motor symptoms. However, longer-term studies are needed to determine whether these physiological gains translate into sustained clinical benefit.
Collectively, the study supports the concept that exercise intensity plays a critical role in optimizing benefit. While both moderate and high-intensity training improve fitness and symptoms, high-intensity intervals appear to produce larger physiological gains in a shorter time frame. For individuals with Parkinson’s disease, this has meaningful implications for exercise prescription and reinforces the importance of including appropriately scaled higher-intensity efforts within training programs.
In Summary
What we find throughout all three studies reinforces a consistent message: exercise is not simply supportive care in Parkinson’s disease, but a biologically meaningful intervention capable of influencing both physiological capacity and brain function. Improvements in cardiorespiratory fitness, reductions in motor symptom severity, and measurable increases in dopamine transporter availability and neuromelanin signal suggest that structured, sufficiently intense exercise has the potential to exert neuromodulatory effects in early disease. Intensity, consistency, and program design appear to matter.
Importantly, the exercise model used in the de Laat et al. (2024) study was not an abstract laboratory construct. Participants completed the Beat Parkinson’s Today program, a community-based, high-intensity interval training model founded by Michelle Hespeler, who was diagnosed with Parkinson’s disease at age 40. Beat Parkinson’s Today integrates interval-based aerobic conditioning, strength training, power development, boxing, balance work, and flexibility training within small-group sessions. Workouts are individualized, scalable, and supervised, emphasizing both relative intensity and safety. Attendance is tracked, feedback is continuous, and the program fosters a strong community bond to promote adherence.
This structure mirrors many foundational principles of CrossFit methodology. CrossFit programming similarly combines aerobic intervals, resistance training, coordination, balance, and functional movement patterns within a scalable framework. Both models emphasize relative intensity rather than absolute load, allowing individuals with varying abilities to train in the same environment. The design of Beat Parkinson’s Today, which served as the intervention in the de Laat study, demonstrates that a similarly CrossFit-aligned structure can be implemented safely in individuals with early Parkinson’s disease while producing measurable neurobiological changes.
Hespeler’s leadership further strengthens the bridge between research and practice. Featured on the CrossFit Podcast, she has described how her program emerged from personal trial and error, participation in clinical trials, and collaboration with academic researchers. What began as a local initiative expanded into multiple locations and online offerings, serving individuals across the United States. Her lived experience shaped a model now supported by emerging imaging data demonstrating increases in dopamine transporter availability and neuromelanin concentration following sustained high-intensity training (de Laat et al., 2024).
The convergence of these elements is notable. A program born from patient advocacy and community implementation was rigorous enough to serve as the intervention in a neuroimaging study demonstrating an improvement in biomarkers associated with dopamine function compared to the expected decline. This linkage underscores an important point: community-based, intensity-driven training models are not outside the scope of scientific medicine. When structured appropriately, they may align directly with mechanisms identified in controlled research.
Within CrossFit affiliates, similar stories have unfolded. Individuals such as Jules King have progressed from requiring full-time assistance and wheelchair use to regaining strength, mobility, and independence through consistent high-intensity functional training. While anecdotal accounts do not replace randomized trials, they provide lived examples that mirror the mechanistic findings emerging in the literature. Improvements in VO₂peak, strength, coordination, and confidence translate into tangible gains in autonomy.
The synthesis of research and real-world experience offers a powerful framework. Imaging studies clarify that dopaminergic systems remain responsive in early disease. Clinical trials demonstrate that cardiorespiratory fitness can improve with higher-intensity training. Community-based programs show that these models are feasible, scalable, and sustainable. Bridging data with compelling narratives may be one of the most effective strategies for reaching individuals with Parkinson’s disease who stand to benefit from structured, high-intensity exercise.
Exercise, when delivered with sufficient intensity and within a supportive environment under the guidance of a knowledgeable trainer, appears capable of influencing both function and neurobiology. CrossFit-aligned programming models, exemplified by Beat Parkinson’s Today, provide a structured pathway for translating this science into practice.
If you’re a CrossFit coach working with individuals living with Parkinson’s, watch and read these: